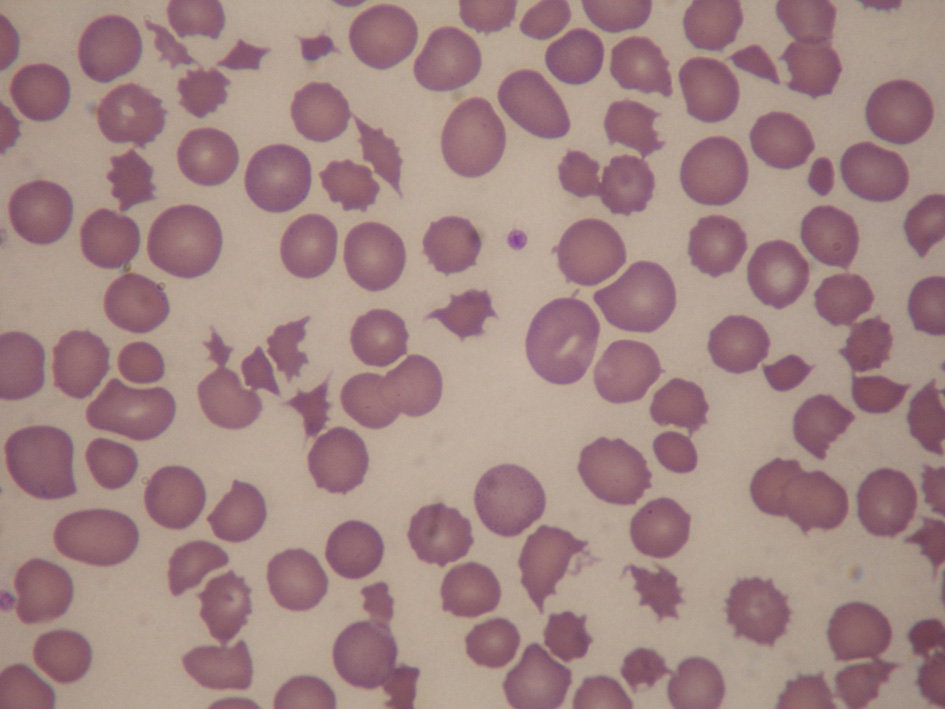
Figure 1. Peripheral blood film showing numerous keratocytes, schistocytes and polychromasia, in keeping with microangiopathic hemolysis.
| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website http://www.thejh.org |
Case Report
Volume 4, Number 4, December 2015, pages 238-241
Diffuse Intrasinusoidal Hepatic Metastasis From Occult Breast Carcinoma Presenting as Thrombotic Microangiopathy: A Case Report and Literature Review
Figures