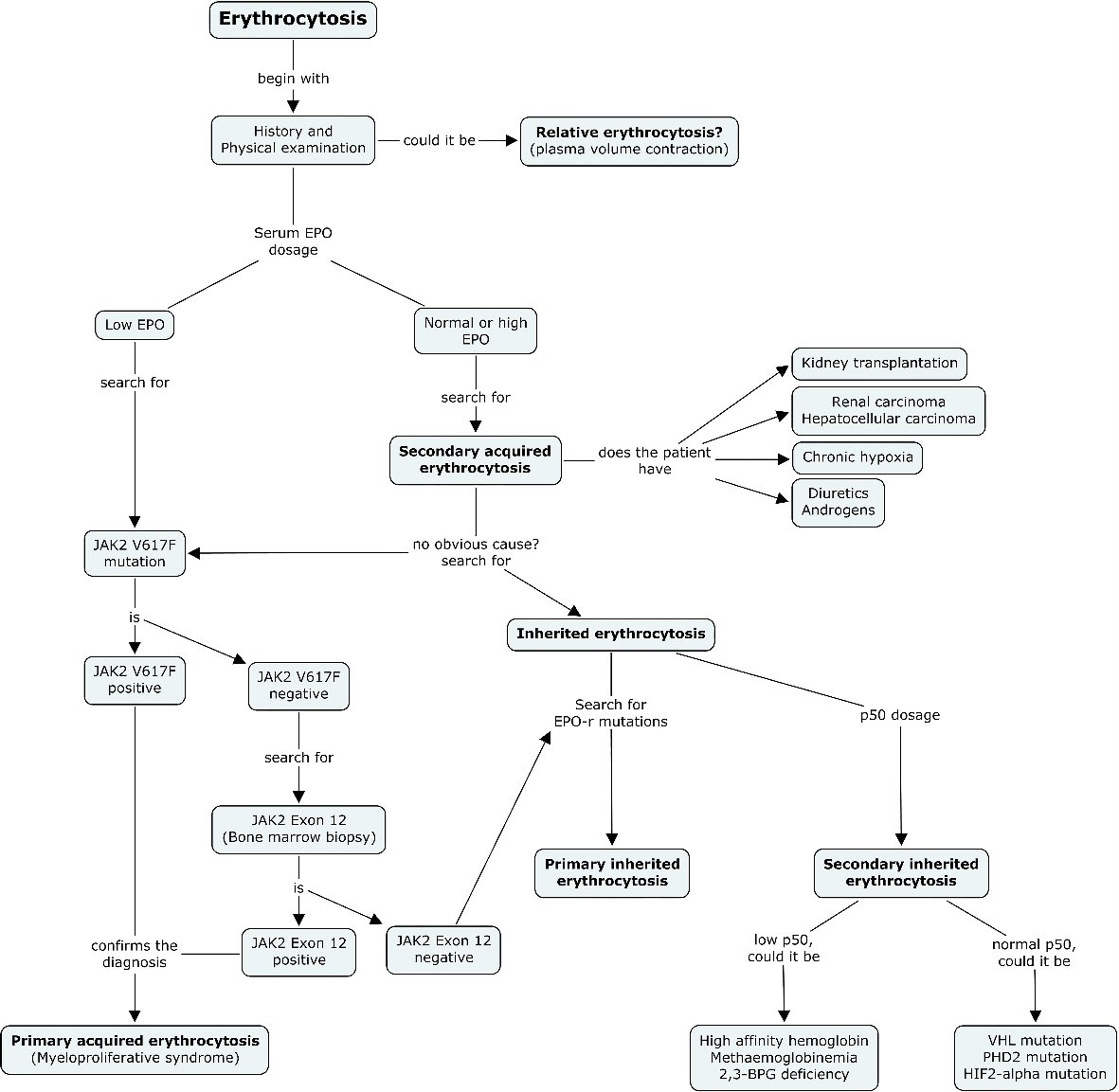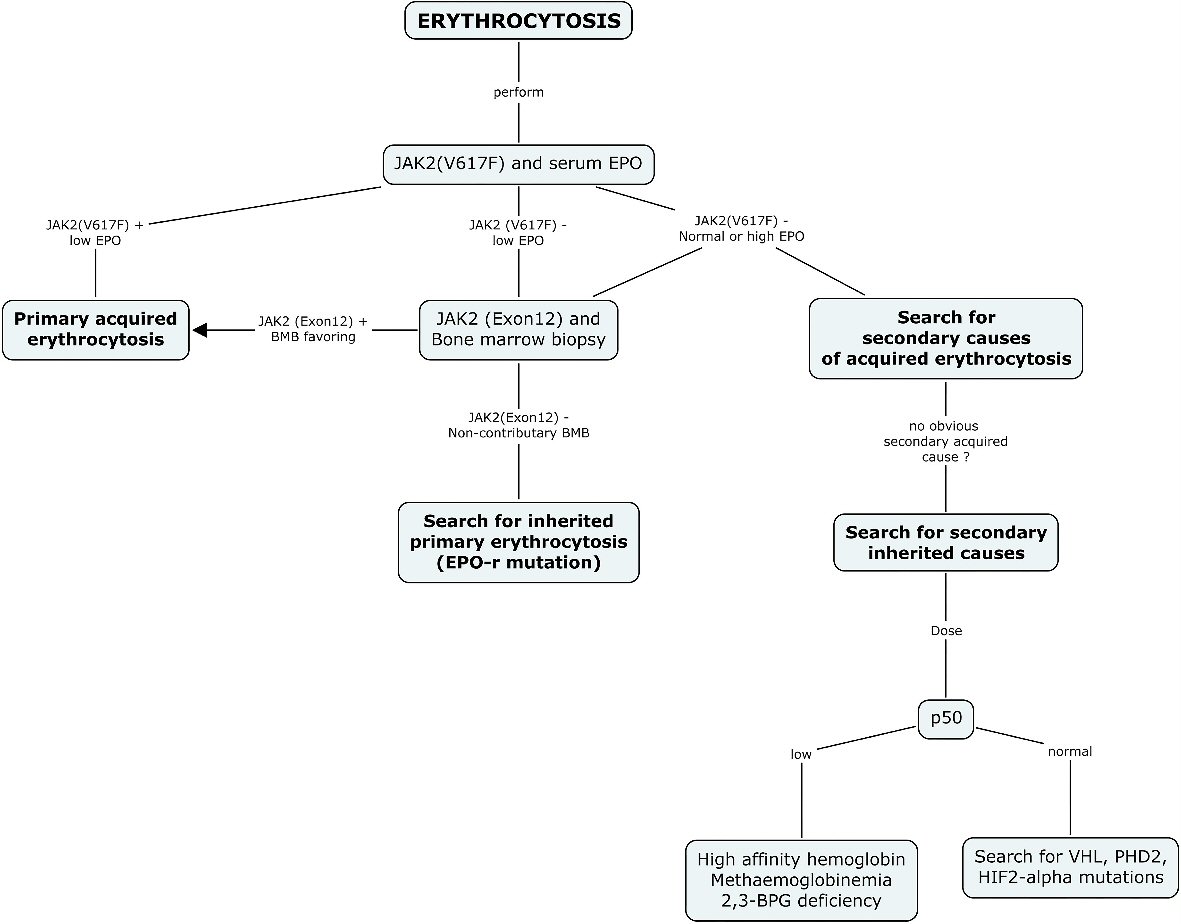
Figure 1. Diagnostic algorithm suggested for erythrocytosis. The current diagnostic approach recommended for the investigation of erythrocytosis systematically includes a search for JAK2 (V617F) mutation and serum EPO as the first step in every patient. A positive JAK2 (V617F) result should orient the diagnosis and management towards a diagnosis of primary acquired erythrocytosis. A normal or high EPO should guide the clinician towards the search for a secondary cause of acquired erythrocytosis, and when no cause is found, the search for a secondary inherited cause. A negative result for JAK2 (V617F) mutation and a low EPO level should be further investigated with a bone marrow biopsy and a search for JAK2 (exon12), and when non-contributory, should prompt a search for inherited primary erythrocytosis. EPO: erythropoietin; BPG: bisphosphoglycerate; HIF-2: hypoxia inducible factor 2; PHD2: prolyl hydroxylase domain protein 2; VHL: von Hippel-Lindau.