

| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website http://www.thejh.org |
Case Report
Volume 4, Number 4, December 2015, pages 228-230
Mobile Thrombus in the Ascending Aorta Associated With Acute Myocardial Infarction
Anthony Lemairea, b, Gregory Maniatisa, Tudor Vagaonescua, Abel Moreyraa, Leonard Y. Leea
aDivision of Cardiothoracic Surgery, Department of Surgery, Rutgers-Robert Wood Johnson Medical School, 125 Paterson Street, New Brunswick, NJ 08903, USA
bCorresponding Author: Anthony Lemaire, Division of Cardiothoracic Surgery, Department of Surgery, Rutgers-Robert Wood Johnson Medical School, 125 Paterson Street, New Brunswick, NJ 08903, USA
Manuscript accepted for publication July 23, 2015
Short title: Mobile Thrombus in the Ascending Aorta
doi: http://dx.doi.org/10.14740/jh201w
| Abstract | ▴Top |
The presence of thrombus in the ascending aorta is uncommon but it has been implicated in systemic thromboembolism. The rarity of thrombus in the ascending aorta is presumably secondary to high blood flow velocity in the location; however, its presence is of concern given the risk of embolization to the brain and potential for cerebral infarction. Furthermore, thrombus in the proximal aorta may embolize into the coronary artery or occlude the coronary ostium and result in myocardial infarction.
Keywords: Thrombus; Myocardial infarction; Ascending aorta
| Introduction | ▴Top |
The presence of thrombus in the ascending aorta is uncommon but has been implicated in systemic thromboembolism [1]. The rarity of thrombus in the ascending aorta is presumably secondary to high blood flow velocity in this location; however, its presence is of concern given the risk of embolization to the brain and potential for cerebral infarction [2]. Furthermore, thrombus in the proximal aorta may embolize into a coronary artery or occlude a coronary ostium and result in myocardial infarction. This is an exceedingly rare clinical occurrence. We present a case of myocardial infarction (MI) caused by occlusion of the left coronary ostium by a mobile aortic thrombus in the absence of associated aortic pathology. We then compare our patient to other cases in the literature.
| Case Report | ▴Top |
A 46-year-old Mongolian female presented with syncope secondary to self-limited episodes of ventricular tachycardia observed in the field. She was a long-standing one-half pack-per-day cigarette smoker without medical comorbidities. Her family history was notable for her mother having a deep venous thrombosis and dying suddenly in her forties. In the emergency room, she was hemodynamically stable with complaints of substernal chest pain. Initial EKG revealed atrial fibrillation with an acute septal infarct and marked inferior ST-depressions. She underwent cardiac catheterization which revealed normal coronary arteries. On exam, she had right lower extremity ischemia with occlusion of the common iliac and popliteal arteries demonstrated on computerized tomography scan.
Her initial echocardiogram revealed severe hypokinesis to akinesis of all myocardial segments except for the basal and mid inferior walls. These findings were confirmed by cardiac magnetic resonance imaging which showed transmural infarction with delayed contrast enhancement of much of the left coronary artery territory. In addition, a 0.4 × 1 cm pedunculated filling defect in the left coronary cusp was identified. The patient’s initial ventriculogram was re-evaluated and a mobile mass was noted above the sinotubular junction unrelated to the aortic valve and close to the ostium of the left main coronary artery.
The mass was presumed to be a thrombus and a cardiothoracic surgical consultation was requested for thrombectomy. The patient was taken to the operating room and an intraoperative echocardiogram demonstrated a mobile mass (Fig. 1). A transverse aortotomy was made in the proximal aorta and an irregular mass was found attached by a thin stalk to the posterior surface of the aorta proximal to the sinotubular junction (Fig. 2). The ascending aorta was otherwise normal without intimal defect or atheroma. The patient was weaned from cardiopulmonary bypass and recovered well postoperatively. Pathology confirmed a pink-red 2.0 × 0.5 cm benign organizing thrombus (Fig. 3). The patient later underwent surgical thrombectomy of her right common iliac and popliteal arteries. She was ultimately discharged in stable condition on standard heart failure medications.
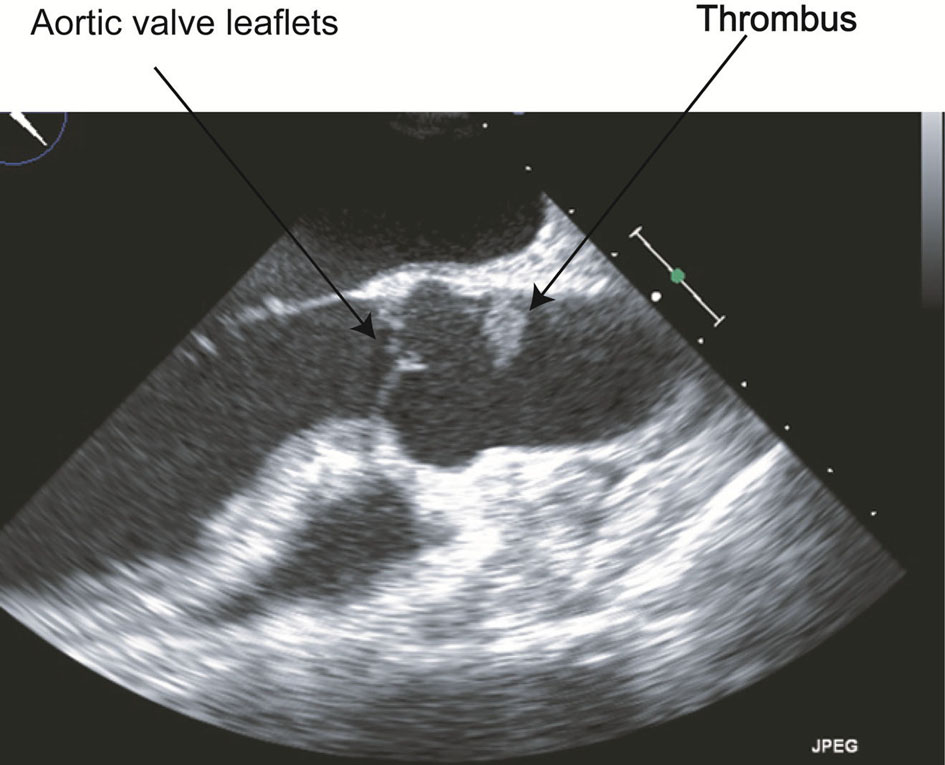 Click for large image | Figure 1. An intraoperative transesophageal echocardiogram view of the aortic thrombus. |
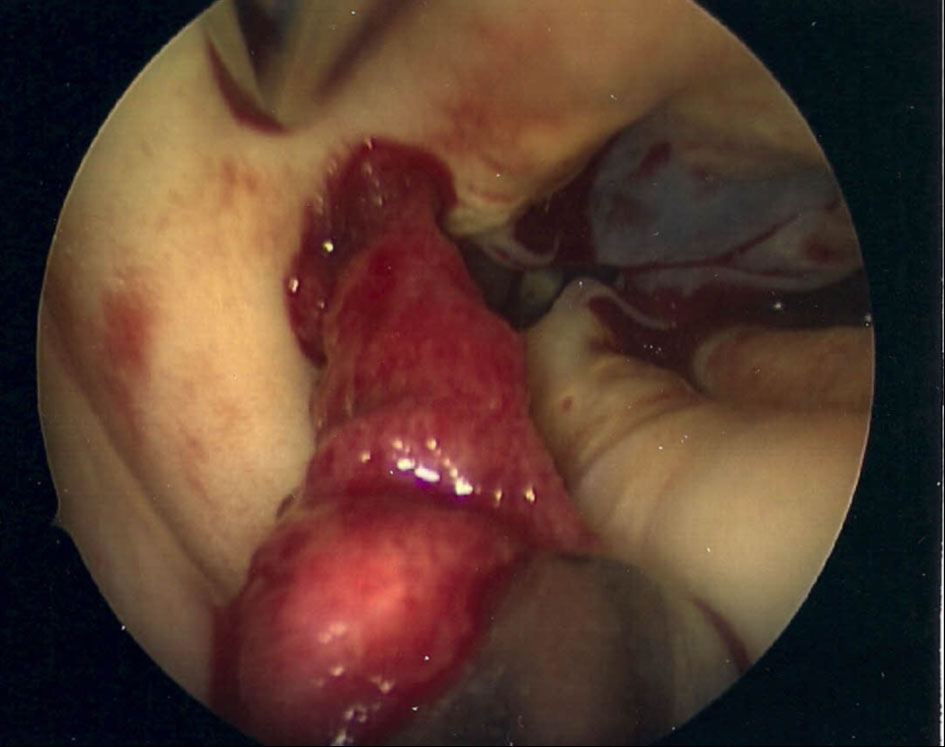 Click for large image | Figure 2. Thrombus within the ascending aorta. |
 Click for large image | Figure 3. Aortic thrombus specimen. |
| Discussion | ▴Top |
Our patient suffered an acute MI in the territory supplied by the left main coronary artery. Immediate cardiac catheterization demonstrated TIMI III blood flow without evidence of atherosclerosis or coronary embolus. Therefore, there was likely temporary occlusion of the left coronary ostium by the mobile aortic thrombus. Aortic thrombosis of the descending aorta is fairly common and usually associated with underlying atherosclerosis or aneurysm. Acute MI secondary to coronary occlusion by a free floating thrombus in the ascending aorta is uncommon. A search of the literature identified only 18 previously reported cases in the absence of other aortic pathology [3-18]. These cases demonstrate that primary thrombus formation can occur in high-flow vascular areas in the absence of obvious aortic pathology. A hypercoagulable workup was performed and significant for an elevated lipoprotein-A level. Of unclear significance, her ANA titer was elevated (1:2,560).
MI secondary to free floating aortic thrombus seems to be more common in young female smokers like our patient. Out of 18 cases identified in the literature, 13 (72%) were female with a mean age of 45 years old, and 57% had a history of cigarette smoking [3-6, 9-11, 13, 15, 16, 18]. Similar to our patient, one other female was found to have an elevated lipoprotein-A level [16]. One male patient was found to have protein S deficiency [12]. Amongst the female patients, one was pregnant [3], and three were known to have been on oral contraceptive or hormone replacement therapy [6, 9, 10]. Like our patient, two others additionally had acute limb ischemia [8, 14].
The mortality associated with MI secondary to free floating aortic thrombus is high (42% in the reviewed cases). The treatment options include anticoagulation with heparin and warfarin [19], thrombolysis [20], and surgical thrombectomy. In this case, we chose surgical intervention to prevent embolization and further occlusion of the coronary ostia.
Conclusion
The presence of aortic thrombus is a rare occurrence and the potential complications from it are severe. In this patient, the thrombus was associated with MI; however, the additional risks include cerebral and/or peripheral embolization. The treatment options are varied but careful management is critical in these patients.
| References | ▴Top |
- Jaworski L, Fijalkowski M, Rogowski J. Giant thrombus in ascending aorta and aortic arch. J Thorac Cardiovasc Surg. 2013;145(6):1668-1669.
doi pubmed - Madershahian N, Kuhn-Regnier F, Mime LB, Slottosch I, Langebartels G, Sindhu D, Wahlers T. A loose cannon: free-floating thrombus in ascending aorta. J Card Surg. 2009;24(2):198-199.
doi pubmed - Knoess M, Otto M, Kracht T, Neis P. Two consecutive fatal cases of acute myocardial infarction caused by free floating thrombus in the ascending aorta and review of literature. Forensic Sci Int. 2007;171(1):78-83.
doi pubmed - Wolfsohn AL, So DY, Chan K, Burwash I, Hendry P, Veinot JP, Labinaz M. Thrombus of the ascending aorta: a rare cause of myocardial infarction. Cardiovasc Pathol. 2005;14(4):214-218.
doi pubmed - Nader RG, Barr F, Rubin R, Hirshfeld JW, Jr., Eisen HJ, Laposata E. Aortic degenerative changes and thrombus formation: an unusual cause of massive myocardial infarction with normal coronary arteries. Am J Med. 1989;86(6 Pt 1):718-722.
doi - Dik H, Hellemans I. An unusual cause of myocardial infarction? Eur Heart J. 1993;14(3):428-430.
doi pubmed - Decker PJ, Scott CH, Fishman LS, Sutton MS. A rare case of coronary artery occlusion diagnosed by echocardiography. Am J Cardiol. 1995;75(1):104-105.
doi - Christiaens L, Allal J, Corbi P. Thrombus in a normal sinus of Valsalva: angiographic, multiplane transoesophageal echocardiographic, and surgical findings. Heart. 1996;76(3):287-288.
doi pubmed - Bruno P, Massetti M, Babatasi G, Khayat A. Catastrophic consequences of a free floating thrombus in ascending aorta. Eur J Cardiothorac Surg. 2001;19(1):99-101.
doi - Ito H, Takahashi K, Sasaki H, Akiho H, Katahira Y, Saito H, Ishibashi T. Large thrombus in the ascending aorta successfully treated by thrombolysis--an unusual cause of acute massive myocardial infarction. Jpn Circ J. 2001;65(6):572-574.
doi pubmed - Shahin GM, Bosker HA, Knaepen PJ, Morshuis WJ, Lindeboom JE. Organized thrombus in the ascending aorta originating from the ostium of the right coronary artery. Cardiovasc Surg. 2002;10(1):62-64.
doi - Eguchi K, Ohtaki E, Misu K, Aikawa M, Sumiyoshi T, Hosoda S, Koyanagi T. Acute myocardial infarction caused by embolism of thrombus in the right coronary sinus of Valsalva: a case report and review of the literature. J Am Soc Echocardiogr. 2004;17(2):173-177.
doi pubmed - Jaafari A, Benyoussef S, Selmi K, Boukhriss B, Boujneh MR. [Myocardial infarction associated with stroke revealing a thrombus of the ascending aorta]. Ann Cardiol Angeiol (Paris). 2004;53(2):105-108.
- Nagata Y, Miyamoto T, Komura M, Niwa A, Kawaguchi S, Shirai T, Fujiwara H, et al. Giant organized thrombus in the left sinus of valsalva causing intermittent left coronary obstruction: an unusual case of acute myocardial infarction. Circ J. 2004;68(8):795-798.
doi pubmed - Elsman P, van 't Hof A, de Boer MJ. Coronary occlusion caused by embolisation from a mass in the sinus of Valsalva. Heart. 2002;88(6):614.
doi pubmed - Soyer H, Laudinat JM, Lemaitre C, Pommier JL, Delepine G, Poncet A, Baehrel B, et al. [Recurrent mobile thrombus of the ascending aorta diagnosed by transesophageal echocardiography]. Arch Mal Coeur Vaiss. 1993;86(12):1769-1771.
pubmed - Kobayashi Y, Hirohata A. Left main coronary thrombotic occlusion due to secondary polycythemia in a normal sinus of valsalva. J Invasive Cardiol. 2013;25(8):421-422.
pubmed - Nakamori S, Matsuoka K, Kurita T, Kusagawa H, Katayama Y. Acute myocardial infarction and cardiogenic shock caused by a mobile thrombus in the ascending aorta unassociated with atherosclerosis. Eur Heart J. 2009;30(20):2440.
doi pubmed - Blackshear JL, Jahangir A, Oldenburg WA, Safford RE. Digital embolization from plaque-related thrombus in the thoracic aorta: identification with transesophageal echocardiography and resolution with warfarin therapy. Mayo Clin Proc. 1993;68(3):268-272.
doi - Hausmann D, Gulba D, Bargheer K, Niedermeyer J, Comess KA, Daniel WG. Successful thrombolysis of an aortic-arch thrombus in a patient after mesenteric embolism. N Engl J Med. 1992;327(7):500-501.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.