

| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website http://www.thejh.org |
Original Article
Volume 6, Number 1, March 2017, pages 6-11
Reference Value Profile for Healthy Individuals From the Aljouf region of Saudi Arabia
Abozer Y. Elderderya, b, d, Abdulaziz S. Alshaibana, c
aFaculty of Applied Medical Sciences, Aljouf University, Saudi Arabia
bFaculty of Medicine and Health Sciences, University of El Imam El Mahdi, Sudan
cFaculty of Applied Medical Sciences, King Saud University, Saudi Arabia
dCorresponding Author: Abozer Elderdery, Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, Aljouf University, Saudi Arabia
Manuscript accepted for publication December 22, 2016
Short title: Reference Value Profile for Healthy Individuals
doi: https://doi.org/10.14740/jh316e
| Abstract | ▴Top |
Background: Many factors influence hematological values such as sex, age, ethnic origin, geographic location, season, and genetic disease. The aim of this study was to detect the hematological reference value profile for healthy adults from the Aljouf region of Saudi Arabia.
Methods: The project was carried out on 2,040 healthy individuals, 1,152 males and 888 females, with ages ranging from 17 to 28 years. A group of participants were recruited from the higher secondary schools, university students and premarital centers of Aljouf cities. Hematological reference value profile, hemoglobin (Hb) concentration, red blood cell (RBC) count, RBC indices, white blood cell (WBC) count, differential WBC and platelet (Plt) count were measured. Moreover, a peripheral blood film was prepared in order to detect abnormalities of RBC and all samples were examined for liver function tests (LFTs) and renal function test (RFT) performed, along with a lipid profile.
Results: Hb concentration, hematocrit (Hct) and RBCs were found to be significantly higher in males than in females (P < 0.01). On the contrary, Plt ranges were significantly lower in male as compared to female (P < 0.01). No significant differences in the study population were determined in the other hematological parameters (P > 0.05).
Conclusion: Our findings reflect that healthy adults from the Aljouf region have some hematological parameters differing quantitatively from Caucasians. The hematological reference value profile reported here can be used as normal reference values for Saudi people of the Aljouf region to help in diagnosis and consequently treatment of individuals with hematological disorders.
Keywords: Full blood count; Hematological parameters; Aljouf
| Introduction | ▴Top |
Many factors influence hematological values such as sex, age, ethnic origin, geographic location, season, and genetic disease [1, 2]. Moreover, a major problem in Arab countries is to determine “normal healthy individuals” due to the high prevalence of hemoglobin (Hb) disorders, iron deficiency anemia and viral infections [3-5]. It is important to recognize that reference ranges in your laboratory may be different; when interpreting results from patients in your laboratory, you must use your own local reference ranges. Thus, unsuitable reference values of hematological profile might elevate the risk of either unessential further investigations or failure to determine underlying disease [6].
Full blood count can be performed either manually or on an automated hematology analyzer, using well mixed anticoagulated (normally EDTA) whole blood. The latter was preferred to be used here, as it is rapid, precise and accurate [7]. This will obviously assist to establish hematological reference values in a proper way.
There are no studies published to date investigating the reference values of hematological profile for healthy individuals in Arab populations in Saudi Arabia. The Saudi Arabs are a distinctive lineage and they live in a particular environment. Also, they have a characteristic lifestyle [8] and they might not be the same as the other population. Therefore, the aim of this study was to detect the hematological reference value profile for healthy adults from the Aljouf region of Saudi Arabia.
Studies of this type are essential to establish hematological reference values which may serve Arabic countries particularly the Aljouf region of Saudi Arabia for interpretation of laboratory results. This will improve and help in diagnosis and treatment of individuals with hematological disorders. The hematological reference values from Aljouf may also serve as a pattern for other Arabic regions, better than the commonly used Caucasian values.
| Materials and Methods | ▴Top |
Hematological parameters and blood morphology, two enzymes (aspartate aminotransferase (AST) and alanine aminotransferase (ALT)) for liver function tests (LFTs), urea and creatinine for renal function test (RFT), along with a lipid profile (total cholesterol and triglyceride), were performed on 1,152 male and 888 female healthy individuals of the Aljouf region, 2,040 in total with ages ranging from 17 to 28 years. Exclusions included those already on medications for anemia and other diseases, smokers and pregnant or lactating individuals.
Participants were recruited from the higher secondary schools, university students and premarital centers of Aljouf cities during the period from January 2015 to June 2016. Ethical approval for the study protocol was obtained from the Faculty of Medical Applied Science, University of Aljouf. Informed consent was obtained individually from all subjects.
Hematological reference value profile, Hb concentration, red blood cell (RBC), RBC indices (packed cell volume (PCV), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC) and red cell distribution width (RDW)), white blood cell (WBC), differential WBC (neutrophil, lymphocyte, monocyte, eosinophil and basophil) and platelet (Plt) count were measured, using a hematology analyzer, BS-320. Moreover, a peripheral blood film was prepared in order to detect abnormalities of RBC, using Leishman’s stain and all samples were examined for ALT and AST as LFT, urea and creatinine as RFT performed, along with total cholesterol and triglyceride as a lipid profile, using chemistry analyzer BS-200.
| Results | ▴Top |
The complete hemogram of the normal adults of Aljouf region is summarized in Table 1. This table also shows comparative statistics between genders. Hb concentration, hematocrit (Hct) and RBCs were found to be significantly higher in males than in females (P < 0.01), as shown in Figure 1a, b and c, respectively. On the contrary, Plt ranges were significantly lower in male as compared to female (P < 0.01) as summarized in Figure 1d.
 Click to view | Table 1. Hematological Reference Value Profile for Normal Adults of Aljouf Region Expressed as a Mean ± SD (95% Range) |
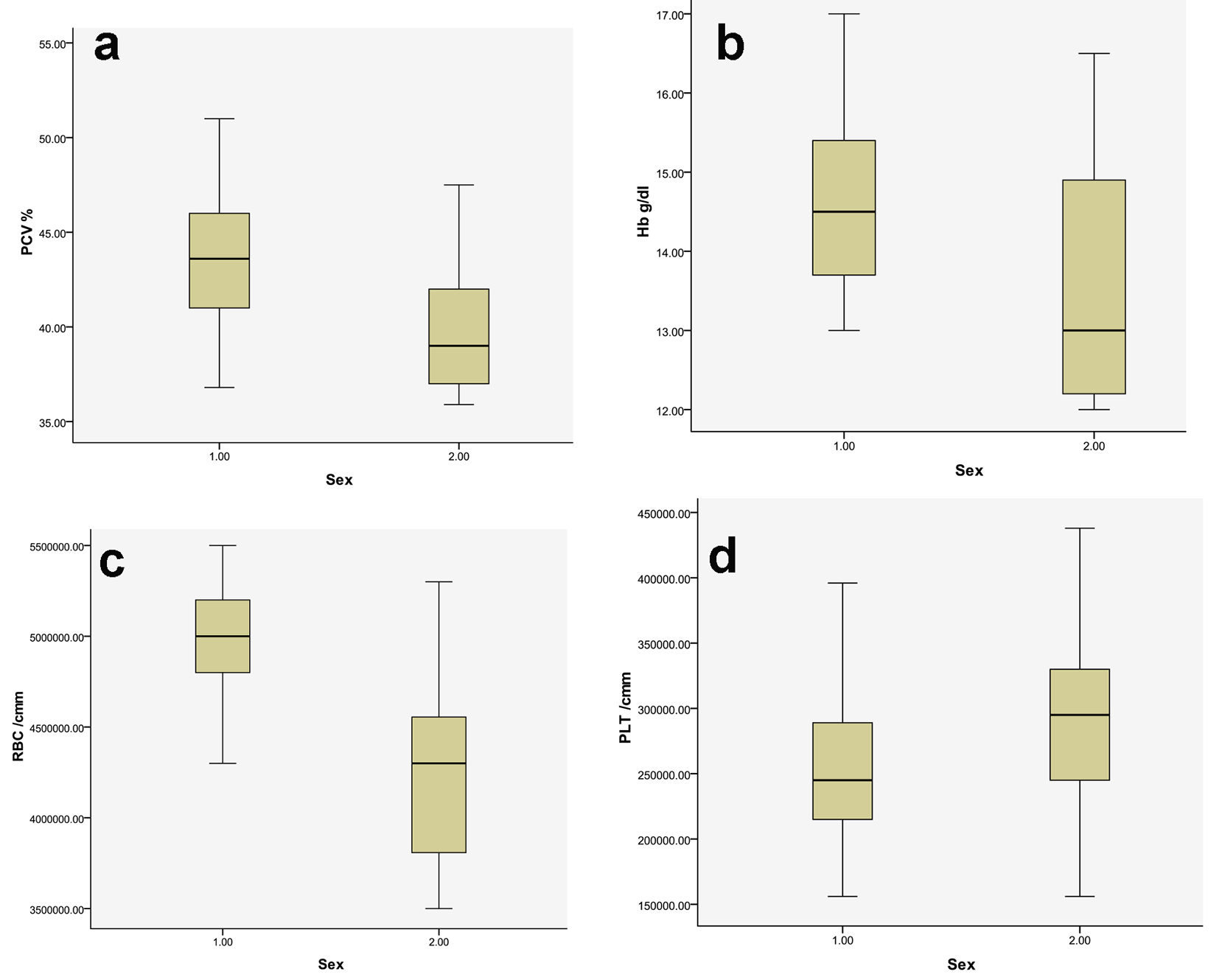 Click for large image | Figure 1. Hematological parameters with significant variation between male and female. PCV: packed cell volume; Hb: hemoglobin; RBC: red blood cell; 1: male; 2: female. |
No significant differences in the study population were determined in the other hematological parameters, RBC indices, WBC and differential WBC count (neutrophil, lymphocyte, monocyte, eosinophil and basophil) (P > 0.05) (Fig. 2). In contrast, our findings reflect that healthy adults from the Aljouf region have some hematological parameters differing quantitatively from Caucasians, as observed in the results of WBC and MCV, while other hematological parameters have reference value profiles which are similar.
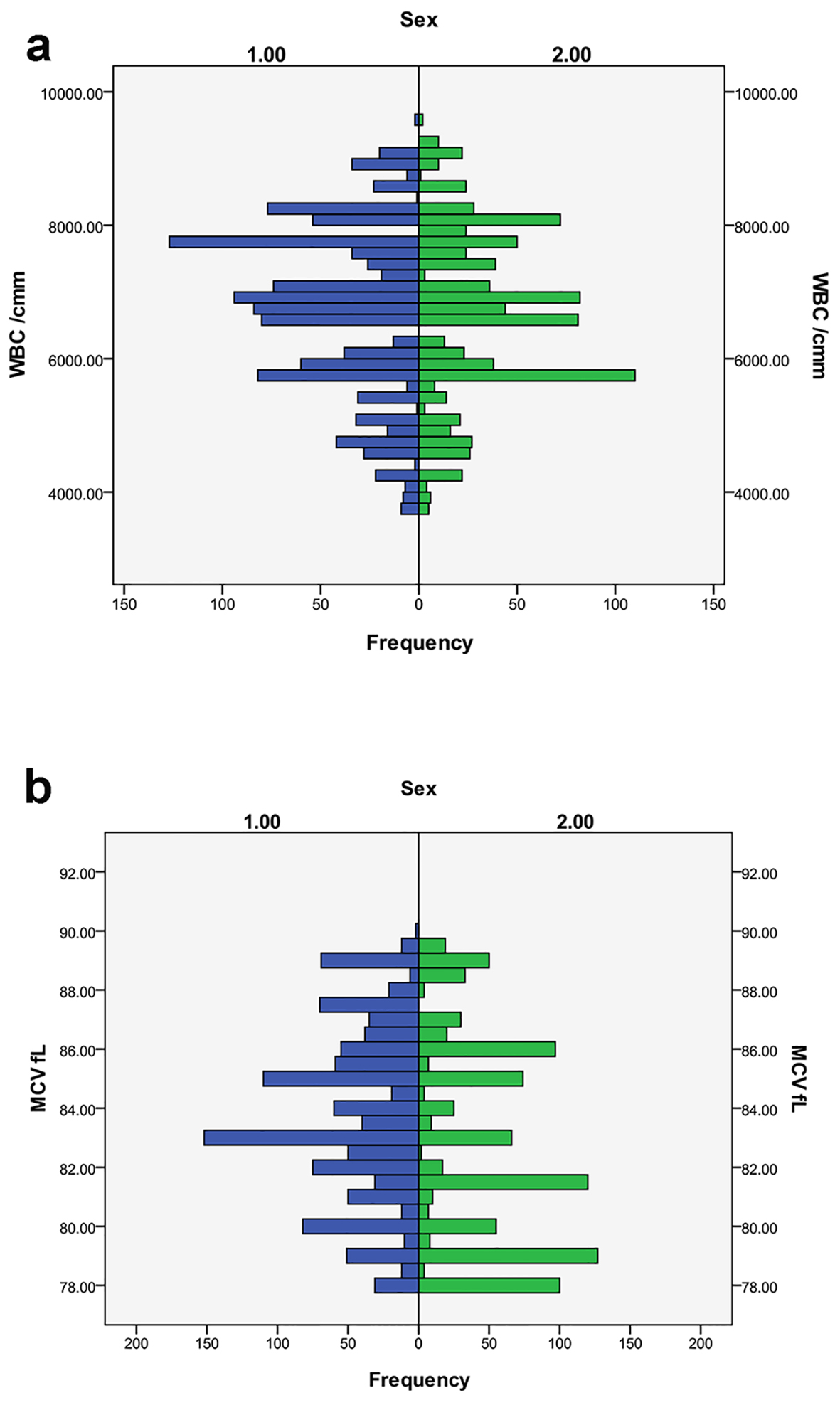 Click for large image | Figure 2. Hematological parameters which do not show significant variation between male and female. WBC: white blood cell; MCV: mean cell volume; 1: male; 2: female. |
The findings in healthy individuals for AST, ALT, urea, creatinine, total cholesterol and triglyceride were within the published normal ranges of 21 (5 ± SD) and 30 (7 ± SD), respectively.
| Discussion | ▴Top |
This is a prospective cross-sectional study to assess the hematological reference value profile, which included differentially counting blood cell types, blood cell morphology and RBC indices. The results incorporate RBC, WBC and Plt counts. The RBC indices contain parameters such as Hb concentration, PCV, MCV, MCH, MCHC and RDW [9]. All these were done in the current study for healthy individuals from the Aljouf region of Saudi Arabia.
Moreover, prior to selecting our participants for hematological reference value profile, an interview and questionnaire was applied to collect demographics: nationality, age, sex, geographical area, family history and clinical data from each participant, because they have a clear role in changing hematological parameters [2]. Other biochemical parameters and risk factors were also considered in selecting healthy individuals for this study. For example, ALT, AST, urea and creatinine were measured to check the function of liver and kidney (Table 2), as these organs are the main sites in producing hemopoietic growth factors such as erythropoietin and thrombopoietin [10, 11]. Total cholesterol and triglyceride were also investigated, because IDA is associated by alteration in these parameters, which responds to iron treatment [12] and other anemia as well [13, 14]. Participants who were diabetic, smoking, pregnant or lactating were also excluded from the study, as they cause alteration in hematological parameters [15-18].
Click to view | Table 2. Clinical Chemistry Parameters for Normal Adults of Aljouf Region Expressed as a Mean ± SD (95% Range) |
Table 1 shows the normal values of each parameter in adults (male and female) and demonstrated significant variations in males versus females as reported in the previous studies [19, 20]. Our results showed that Hb concentration, Hct and RBCs were found to be significantly higher in males than in females (P < 0.01). This is expected to be found among the study population, which is similar to the studies carried out in the developed countries, Arab countries [21], Asian countries [22, 23] and also comparable to documentation from Africa [19, 23].
On the contrary, Plt ranges were significantly lower in male as compared to female, which is in agreement with the other reported studies [19, 20, 22]. This may be as a result of the differences in hormone types and concentrations in the different sexes and the consequence of thrombopoietin release in response to regular menstruation cross-stimulating thrombopoiesis. In fact, the main cause for these lower values is still unknown and therefore further research is essential. However, other studies documented that these lower values might be due to the diet, genetic factors or other environmental factors [24].
In contrast, the Plt counts and MCV values are lower in comparison with the Caucasians, USA values and other African studies [19, 20]. Our findings reflect that healthy adults from the Aljouf region have also some hematological parameters differing quantitatively from Arab [19, 21], Caucasians [25, 26], Asian [23, 27] and African [20, 28, 29], while other hematological parameters have reference value profiles which are similar to these ethnic groups [18, 20, 21, 23, 26, 27, 29].
It is of interest to report also that the reference values of MCV and WBC from the current study were on most occasions far lower than those of other European countries [25]. Similar results of MCV, WBC, Hb, PCV and RBC with varying degrees have been made in studies carried out in other ethnic groups such as Palestine [21], Tanzania [19], Sudan [28], Kenya [29], Nigeria, and Turkey [30].
Conclusion
Our findings reflect that healthy adults from the Aljouf region have some hematological parameters differing quantitatively from Caucasians, while other hematological parameters have reference value profiles which are similar to Caucasians. Therefore, hematological reference value profile reported in this study can be used as normal reference values for Saudi people of the Aljouf region to improve and help in diagnosis and treatment of individuals with hematological disorders.
Acknowledgments
The authors thank individuals for their participation. Thanks to our colleagues, Mr. Abdelgadir Ahmed and Mr. Atif Elrais for their assistance and university students of Aljouf University for their participation and this study. We would like also to thank staff and administration of the higher secondary schools, and premarital centres of Aljouf cities for their cooperation. The authors are thankful to the Deanship of Scientific Research and postgraduate studies, Aljouf University for funding the work through the research group project No. 35/4342.
| References | ▴Top |
- Bain B, Seed M, Godsland I. Normal values for peripheral blood white cell counts in women of four different ethnic origins. J Clin Pathol. 1984;37(2):188-193.
doi pubmed - Verma U, Shankar N, Madhu SV, Tandon OP, Madan N, Verma N. Relationship between iron deficiency anaemia and serum lipid levels in Indian adults. J Indian Med Assoc. 2010;108(9):555-558, 562.
pubmed - Al Hawsawi ZM, Al-Rehali SA, Mahros AM, Al-Sisi AM, Al-Harbi KD, Yousef AM. High prevalence of iron deficiency anemia in infants attending a well-baby clinic in northwestern Saudi Arabia. Saudi Med J. 2015;36(9):1067-1070.
doi pubmed - Alsultan A, Alabdulaali MK, Griffin PJ, Alsuliman AM, Ghabbour HA, Sebastiani P, Albuali WH, et al. Sickle cell disease in Saudi Arabia: the phenotype in adults with the Arab-Indian haplotype is not benign. Br J Haematol. 2014;164(4):597-604.
doi pubmed - Alquaiz AM, Gad Mohamed A, Khoja TA, Alsharif A, Shaikh SA, Al Mane H, Aldiris A, et al. Prevalence of anemia and associated factors in child bearing age women in riyadh, saudi arabia. J Nutr Metab. 2013;2013:636585.
doi pubmed - Taouinet R, Mougin G, Brun C, Darodes de Tailly P. [Statistical comparison of the results of the blood cells count obtained with a Micros 60 ABX analyzer using the genuine reagents and generics reagents kits]. Ann Biol Clin (Paris). 2007;65(6):671-676.
- Kawai Y, Takeuchi K, Shimizu N, Uehara S, Nakayama Y, Mitsuhashi T, Watanabe K. [Accuracy, precision and clinically acceptable level of complete blood cell count by an automated multichannel hematology analyzer]. Rinsho Byori. 1999;47(4):343-352.
pubmed - Hassan NNA. High prevalence of iron deficiency anemia in infants attending a well-baby clinic in northwestern Saudi Arabia. Journal of Microscopy and Ultrastructure. 2015;3(1):25-28.
- Clarke GM, Higgins TN. Laboratory investigation of hemoglobinopathies and thalassemias: review and update. Clin Chem. 2000;46(8 Pt 2):1284-1290.
pubmed - Sharples EJ, Thiemermann C, Yaqoob MM. Novel applications of recombinant erythropoietin. Curr Opin Pharmacol. 2006;6(2):184-189.
doi pubmed - Marconi GD, Zara S, De Colli M, Di Valerio V, Rapino M, Zaramella P, Dedja A, et al. Postnatal hyperoxia exposure differentially affects hepatocytes and liver haemopoietic cells in newborn rats. PLoS One. 2014;9(8):e105005.
doi pubmed - Kumar A. National nutritional anaemia control programme in India. Indian J Public Health. 1999;43(1):3-5, 16.
pubmed - Seip M, Skrede S. Serum cholesterol and triglycerides in children with anaemia. Scand J Haematol. 1977;19(5):503-508.
doi pubmed - el-Hazmi MA, Jabbar FA, Warsy AS. Cholesterol and triglyceride level in patients with sickle cell anaemia. Scand J Clin Lab Invest. 1987;47(4):351-354.
doi pubmed - Bhalla DK, Hirata F, Rishi AK, Gairola CG. Cigarette smoke, inflammation, and lung injury: a mechanistic perspective. J Toxicol Environ Health B Crit Rev. 2009;12(1):45-64.
doi pubmed - Gajda K, Sulich A, Hamulka J, Bialkowska A. Comparing diabetic with non-diabetic overweight subjects through assessing dietary intakes and key parameters of blood biochemistry and haematology. Rocz Panstw Zakl Hig. 2014;65(2):133-138.
pubmed - S AL, Lakshmanan A, P GK, A S. Effect of intensity of cigarette smoking on haematological and lipid parameters. J Clin Diagn Res. 2014;8(7):BC11-13.
- Milman N, Pedersen AN. Blood haemoglobin concentrations are higher in smokers and heavy alcohol consumers than in non-smokers and abstainers: should we adjust the reference range? Ann Hematol. 2009;88(7):687-694.
doi pubmed - Saathoff E, Schneider P, Kleinfeldt V, Geis S, Haule D, Maboko L, Samky E, et al. Laboratory reference values for healthy adults from southern Tanzania. Trop Med Int Health. 2008;13(5):612-625.
doi pubmed - Gelaye B, Bekele T, Khali A, Haddis Y, Lemma S, Berhane Y, Williams MA. Laboratory reference values of complete blood count for apparently healthy adults in Ethiopia. Clin Lab. 2011;57(7-8):635-640.
pubmed - Sirdah MM, Tarazi IS, El Jeadi H, Al Haddad RM. Normal blood cells reference intervals of healthy adults at the Gaza Strip-Palestine. J Clin Lab Anal. 2008;22(5):353-361.
doi pubmed - Ambayya A, Su AT, Osman NH, Nik-Samsudin NR, Khalid K, Chang KM, Sathar J, et al. Haematological reference intervals in a multiethnic population. PLoS One. 2014;9(3):e91968.
doi pubmed - A RS, Parameaswari PJ, Shanthi B, Revathy C, Parijatham BO. The reference intervals for the haematological parameters in healthy adult population of chennai, southern India. J Clin Diagn Res. 2012;6(10):1675-1680.
pubmed - Azikiwe AN. Platelet count values in healthy Nigeria medical students in Jos. East Afr Med J. 1984;61(6):482-485.
pubmed - Wakeman L, Al-Ismail S, Benton A, Beddall A, Gibbs A, Hartnell S, Morris K, et al. Robust, routine haematology reference ranges for healthy adults. Int J Lab Hematol. 2007;29(4):279-283.
doi pubmed - Bain BJ. Ethnic and sex differences in the total and differential white cell count and platelet count. J Clin Pathol. 1996;49(8):664-666.
doi pubmed - Usman K SZ, Rao AA. Reference range values of haematological parameters in healthy Pakistani adults. Pak J Physiol. 2007;(3):19-22.
- Elderdery AY, Mohamed BA, Karsani ME, Ahmed MH, Knight G, Cooper AJ. Hemoglobinopathies in the Sudan. Hemoglobin. 2008;32(3):323-326.
doi pubmed - Kibaya RS, Bautista CT, Sawe FK, Shaffer DN, Sateren WB, Scott PT, Michael NL, et al. Reference ranges for the clinical laboratory derived from a rural population in Kericho, Kenya. PLoS One. 2008;3(10):e3327.
doi pubmed - Nilgun Tekkesin HB, Faruk Tukenmez. The largest reference range study for hematological parameters from Turkey: A case control study. Journal of Clinical and Experimental Investigations. 2014;5(4):548-552.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.