

| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website https://www.thejh.org |
Case Report
Volume 11, Number 2, April 2022, pages 77-80

COVID-19-Associated Pneumonia in a B-Cell-Depleted Patient With Non-Hodgkin Lymphoma: Recovery With Hyperimmune Plasma
Daniele Colomboa, d, Arianna Gattib, Patrizia Alabardia, Daniela Bompanea, Giorgio Bonardia, Nicola Mumolic, Paola Faggiolia, Pierangelo Clericib, Bruno Brandob, Antonino Mazzonea
aInternal Medicine Unit, Legnano Hospital, ASST Ovest Milanese, Legnano (MI), Italy
bHematology Laboratory and Transfusion Center, Legnano Hospital, ASST Ovest Milanese, Legnano (MI), Italy
cInternal Medicine Unit, Magenta Hospital, ASST Ovest Milanese, Magenta (MI), Italy
dCorresponding Author: Daniele Colombo, Internal Medicine Unit, Legnano Hospital, ASST Ovest Milanese, Legnano (MI), Italy
Manuscript submitted April 23, 2021, accepted June 3, 2021, published online April 22, 2022
Short title: Hyperimmune Plasma in B-Cell Depletion in COVID-19
doi: https://doi.org/10.14740/jh845
| Abstract | ▴Top |
Coronavirus disease 2019 (COVID-19) can have a severe course in immunocompromised hosts and patients with hematological malignancies. In some cases, the bad prognosis is associated with the lack of B lymphocytes, with impaired antibody production and inefficient viral clearance. We report a case of a 67-year-old woman with a story of non-Hodgkin lymphoma treated with R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone), who got a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection while being totally depleted of B cells. This condition has determined a severe and prolonged course of COVID-19, with persistently positive nasopharyngeal molecular swabs and lack of anti-SARS-CoV-2 specific antibodies. The clinical recovery was favored by the administration of convalescent hyperimmune plasma.
Keywords: COVID-19; Convalescent plasma; Rituximab; SARS-CoV-2 swab; Anti-SARS-CoV-2 antibodies
| Introduction | ▴Top |
During the coronavirus disease 2019 (COVID-19) pandemic, patients with pre-existing comorbidities and immunosuppression are particularly at risk for severe disease [1, 2]. Patients suffering from hematological malignancies that affect B cells or that require B-cell-depleting treatments are at higher risk and have a poorer prognosis after infection [1-3]. In such patients COVID-19 pneumonia has frequently a severe and prolonged course, with molecular detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in body fluids remaining positive for weeks or months. Patients treated with B-cell-depleting regimens have a hampered antibody production [4], which frequently explains the impaired viral clearance and the unfavorable prognosis of COVID-19.
Recent studies showed that the expression of CD169 on monocytes is a useful marker to diagnose early SARS-CoV-2 infection. CD169 (sialoadhesin or Siglec-1) is a type I interferon-inducible receptor, and its expression is upregulated on monocytes during viral infections, included SARS-CoV-2 [5]. In this study we have used this marker to monitor the response to hyperimmune plasma administration in a B-cell-depleted hematological patient with COVID-19 pneumonia.
| Case Report | ▴Top |
Investigations
A 67-year-old woman had a history of stage IV leukemic non-Hodgkin follicular lymphoma with pleuro-pulmonary and osteomedullary involvement, diagnosed in October 2019. She has been treated with R-CHOP (rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone) until May 2020, followed by a maintenance treatment with bimonthly rituximab 375 mg/m2 (last administration in October 2020). In November 2020 the patient reported fever with interstitial pneumonia, and a nasopharyngeal molecular swab was positive for SARS-CoV-2 RNA. She was admitted to the infectious diseases ward, where she was treated for 15 days with oxygen, remdesivir, heparin and steroids, and discharged thereafter in a satisfactory although incomplete clinical recovery and with a negative molecular nasopharyngeal swab. After a few days, however, fever and low oxygen saturation resumed, so she returned to the emergency department, where a chest computed tomography (CT) scan showed persistence of peripheral ground-glass opacities, with a newly positive molecular swab. She was admitted to another medical ward and treated with methylprednisolone at a 1.5 mg/kg/day dose with a good respiratory improvement, so she was discharged at the end of December 2020, despite a persistently positive molecular swab and the total absence of peripheral B cells. She underwent a whole-body 18F-fluoro-2-deoxy-D-glucose positron emission tomography (18FDG-PET) in January 2021 for lymphoma monitoring, which showed incidentally the persistence of ground-glass opacities in the lungs. Because of recurrent fever, a new admission was needed, and the patient came to our observation on January 8, 2021.
Diagnosis
A bronchoscopy showed the persistence of SARS-CoV-2 RNA in the bronchoalveolar lavage but excluded the reactivation of lymphoma. The patient was treated again with steroids and intravenous immunoglobulin (Ig) 0.4 g/kg for very low serum Ig levels, with resolution of symptoms, despite the persistent positivity of repeated molecular nasopharyngeal swabs. Another flow cytometric analysis of lymphocyte subsets was performed. The high-resolution peripheral lymphocyte immunophenotyping [6] confirmed the absence of B cells, at 0.0025% sensitivity level. The lymphocyte population (700/µL) was composed by T cells (580/µL), with low CD4/CD8 ratio (0.73) and natural killer (NK) cells (119/µL). In addition, CD169 expression on monocyte surface was studied. The monocyte CD169 expression is quantified as the ratio between CD169 intensity on monocytes divided by the CD169 intensity on lymphocytes, which acts as the negative control (Fig. 1). In healthy subjects this ratio is < 10, while in our patient the ratio was 72.7. The patient’s serum showed a low total IgG level (337 mg/dL), was negative for anti-SARS-CoV-2 antibodies but preserved a good serological memory for a previous Epstein-Barr virus (EBV) infection (anti-EBV Epstein-Barr nuclear antigen (EBNA) IgG 278 U/mL, EBV virus capsid antigen (VCA) IgG > 750 U/mL), while positive nasopharyngeal swabs for SARS-CoV-2 RNA were repeatedly found.
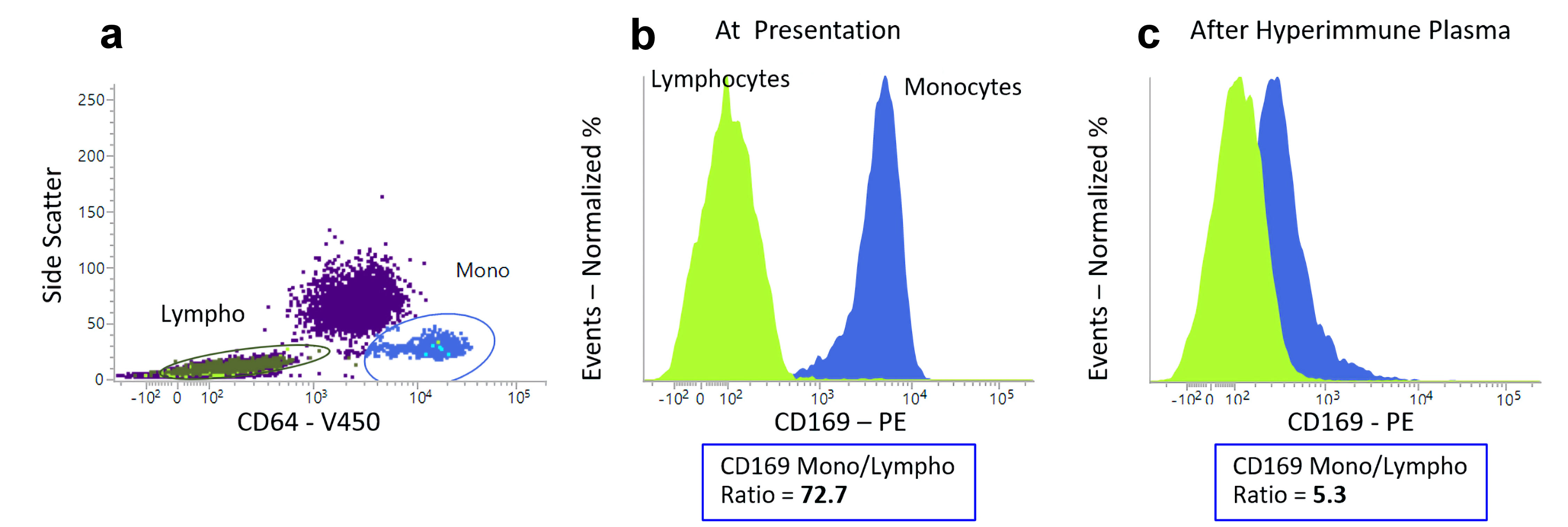 Click for large image | Figure 1. Monocyte CD169 expression during the overt COVID-19 infection and after the clinical recovery obtained with hyperimmune plasma. The reduced CD169 monocyte/lymphocyte ratio at discharge correlates with the viral clearance. (a) Dot plot SSC/CD64. Monocytes (Mono, blue) and lymphocytes (Lympho, green) are identified on the basis of their respective intensity of expression of CD64. (b) The green histogram represents the CD169 intensity on lymphocytes (negative control) and the blue histogram the CD169 intensity on monocytes at presentation with an intensity ratio of 72.7. (c) After hyperimmune plasma treatment, a significant decrease of the ratio was found, indicating viral clearance (5.3). COVID-19: coronavirus disease 2019; SSC: side scatter. |
Treatment
On the basis of these findings, we decided to administer two 300 mL doses of convalescent hyperimmune plasma from the same donor on January 27 and 28, 2021 (as measured in the plasma bags: total anti-SARS-CoV-2 antibodies 559 U (positive cut-off > 1 U); IgG antibodies 8.47 U (positive cut-off > 1 U), Ortho Vitros SARS-CoV-2 kit).
Follow-up and outcomes
Two days after the administration of plasma the nasopharyngeal swab was repeated and resulted negative for SARS-CoV-2 RNA, whereas patient’s serum showed a good level of passive immunization with the presence of 275 U of total anti SARS-COV-2 specific antibodies. The patient was discharged on February 1 in satisfactory clinical conditions, with no fever nor respiratory distress, and remained stable thereafter.
| Discussion | ▴Top |
Several studies showed that patients with hematological diseases are characterized by a dismal prognosis when affected by COVID-19 [1, 2], with prolonged persistence of SARS-CoV-2 RNA in respiratory samples [3]. This seems due to the reduced ability of the host immune response to eradicate the SARS-CoV-2 colonization [7]. The ground glass appearance at chest CT scan is the most frequently observed pattern of lung involvement in these patients [8]. The hematological disorder itself and the related chemotherapy and immunosuppression, especially if induced by rituximab, determine the impaired viral clearance, with frequent superimposed bacterial infections. We observed such occurrences in many oncohematologic patients admitted to our hospital unit, and most of them died. It has been demonstrated that the presence of anti-SARS-CoV-2 nucleocapsid protein (NP) or anti-SARS-CoV-2 receptor-binding domain (RBD) IgG levels in affected patients’ sera correlate with the ability to neutralize the virus [9]. However, most hematological and immunocompromised patients seem unable to build up an efficient antibody response, both to infection and in response to vaccine [10]. In this case report, despite the long exposure to the virus, a patient previously treated with repeated cycles of rituximab and completely depleted of B cells was unable to produce antibodies against SARS-CoV-2 and had a prolonged COVID-19 clinical syndrome (Fig. 2). Convalescent hyperimmune plasma infusion has been studied as a possible therapy for COVID-19, but its efficacy is still controversial in prospective randomized trials [11, 12]. It is reported that antibodies in convalescent plasma may suppress the viral load once passively transferred to immunocompromised hosts [12]. Despite the ongoing controversies and in the absence of other therapeutical options like monoclonal antibodies [13], we decided to treat with convalescent plasma a B-cell-depleted patient at high clinical risk, unable to build up an antibody response to the new infection, while keeping the serologic memory of previous viral challenges [6]. After the hyperimmune plasma infusion the symptoms promptly faded out and the patient achieved the viral eradication. In addition, we monitored a significant reduction of the monocyte CD169 expression (ratio = 5.3 at discharge), further corroborating the achievement of the viral clearance. We have successfully treated two more patients with similar features (underlying hematological malignancies treated with rituximab with no circulating B cells, data not shown), thus supporting the rationale of hyperimmune convalescent plasma use in COVID-19 patients with impaired antibody production and absence of B lymphocytes. Our experience may be considered as the starting point for further studies including a greater cohort of immunocompromised patients.
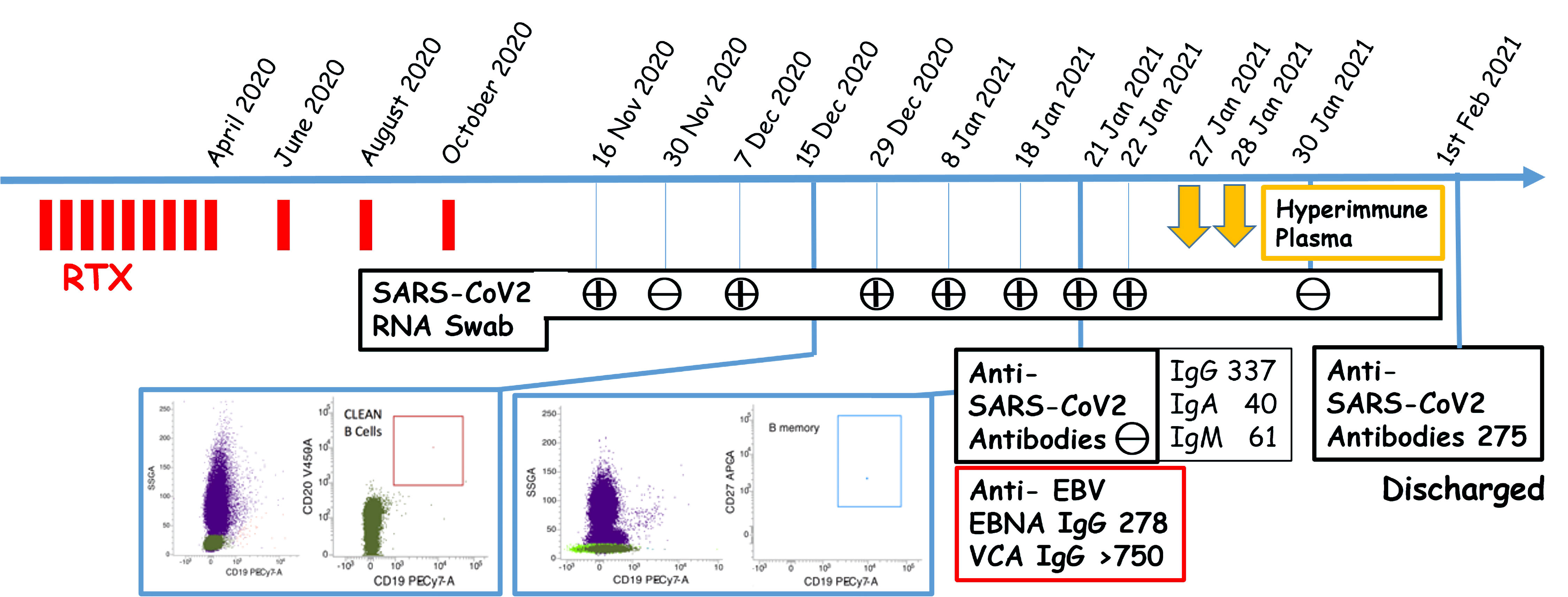 Click for large image | Figure 2. Clinical course. The patient received 12 courses of rituximab (RTX) and remained B-cell-depleted for months, being unable to mount an antibody response against SARS-CoV-2. She remained persistently positive for nasopharyngeal molecular swabs and with pulmonary involvement. Clinical recovery and negativization of molecular swab occurred after the administration of two units of hyperimmune convalescent plasma. SARS-CoV-2: severe acute respiratory syndrome coronavirus 2. |
Since rituximab is widely used also in a number of autoimmune disorders, the SARS-CoV-2 pandemic poses additional challenges in case of the occurrence of COVID-19 infection in patients with autoimmune diseases or transplanted grafts [14, 15].
Hematological patients with superimposed SARS-CoV-2 infection have a high mortality risk, due to the underlying disease and treatment. Currently the use of hyperimmune convalescent plasma is still controversial in the treatment of COVID-19. We think that this treatment may be however useful for B-cell-depleted, severely immunocompromised patients with SARS-CoV-2 infection with proven inability to mount an efficient antibody response.
Acknowledgments
Thanks to Simona Puricelli and Stefania De Rosa, part of our staff.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained.
Author Contributions
Daniele Colombo and Arianna Gatti wrote the article and worked out the idea. Patrizia Alabardi, Daniela Bompane and Giorgio Bonardi followed the patient during the hospitalization. Nicola Mumoli, Paola Faggioli and Pierangelo Clerici elaborated the data. Bruno Brando and Antonino Mazzone reviewed and supervised the entire work.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Lee LY, Cazier JB, Angelis V, Arnold R, Bisht V, Campton NA, Chackathayil J, et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: a prospective cohort study. Lancet. 2020;395(10241):1919-1926.
doi - Sanchez-Pina JM, Rodriguez Rodriguez M, Castro Quismondo N, Gil Manso R, Colmenares R, Gil Alos D, Paciello ML, et al. Clinical course and risk factors for mortality from COVID-19 in patients with haematological malignancies. Eur J Haematol. 2020;105(5):597-607.
doi pubmed - He W, Chen L, Chen L, Yuan G, Fang Y, Chen W, Wu D, et al. COVID-19 in persons with haematological cancers. Leukemia. 2020;34(6):1637-1645.
doi pubmed - Patel SY, Carbone J, Jolles S. The expanding field of secondary antibody deficiency: causes, diagnosis, and management. Front Immunol. 2019;10:33.
doi pubmed - Bedin AS, Makinson A, Picot MC, Mennechet F, Malergue F, Pisoni A, Nyiramigisha E, et al. Monocyte CD169 expression as a biomarker in the early diagnosis of coronavirus disease 2019. J Infect Dis. 2021;223(4):562-567.
doi pubmed - Gatti A, Buccisano F, Scupoli MT, Brando B. The ISCCA flow protocol for the monitoring of anti-CD20 therapies in autoimmune disorders. Cytometry B Clin Cytom. 2021;100(2):194-205.
doi pubmed - Carmo A, Pereira-Vaz J, Mota V, Mendes A, Morais C, da Silva AC, Camilo E, et al. Clearance and persistence of SARS-CoV-2 RNA in patients with COVID-19. J Med Virol. 2020;92(10):2227-2231.
doi pubmed - Cao Y, Liu X, Xiong L, Cai K. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2: A systematic review and meta-analysis. J Med Virol. 2020;92(9):1449-1459.
doi pubmed - To KK, Tsang OT, Leung WS, Tam AR, Wu TC, Lung DC, Yip CC, et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis. 2020;20(5):565-574.
doi - Eisenberg RA, Jawad AF, Boyer J, Maurer K, McDonald K, Prak ET, Sullivan KE. Rituximab-treated patients have a poor response to influenza vaccination. J Clin Immunol. 2013;33(2):388-396.
doi pubmed - Simonovich VA, Burgos Pratx LD, Scibona P, Beruto MV, Vallone MG, Vazquez C, Savoy N, et al. A randomized trial of convalescent plasma in COVID-19 severe pneumonia. N Engl J Med. 2021;384(7):619-629.
doi pubmed - Chen L, Xiong J, Bao L, Shi Y. Convalescent plasma as a potential therapy for COVID-19. Lancet Infect Dis. 2020;20(4):398-400.
doi - Weinreich DM, Sivapalasingam S, Norton T, Ali S, Gao H, Bhore R, Musser BJ, et al. REGN-COV2, a neutralizing antibody cocktail, in outpatients with COVID-19. N Engl J Med. 2021;384(3):238-251.
doi pubmed - Mehta P, Porter JC, Chambers RC, Isenberg DA, Reddy V. B-cell depletion with rituximab in the COVID-19 pandemic: where do we stand? Lancet Rheumatol. 2020;2(10):e589-e590.
doi - Yasuda H, Tsukune Y, Watanabe N, Sugimoto K, Uchimura A, Tateyama M, Miyashita Y, et al. Persistent COVID-19 pneumonia and failure to develop anti-SARS-CoV-2 antibodies during rituximab maintenance therapy for follicular lymphoma. Clin Lymphoma Myeloma Leuk. 2020;20(11):774-776.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.