

| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website http://www.thejh.org |
Short Communication
Volume 8, Number 2, June 2019, pages 55-59
C-Reactive Protein Level: A Key Predictive Marker of Cachexia in Lymphoma and Myeloma Patients
Joris Mallarda, b, Anne-Laure Gagezc, Cedric Baudineta, Aline Herbineta, Jonathan Maurya, Pierre Louis Bernardb, d, Guillaume Cartronc, e, f
aV@Si SAS, Research and Development Department, Montpellier University, 93 Plan de la Prairie, 34270 Saint-Mathieu-de-Treviers, France
bSports Sciences Unity, University of Montpellier, 700 Avenue du Pic Saint-Loup, 34090 Montpellier, France
cDepartment of Clinical Hematology, Montpellier University Hospitality, 80 Avenue Augustin Fliche, 34090 Montpellier, France
dEuromov Laboratory, Montpellier University, 700 Avenue du Pic Saint-Loup, 34090 Montpellier, France
eCNRS UMR 5235, University of Montpellier, Montpellier, France
fCorresponding Author: Guillaume Cartron, Departement d’Hematologie Clinique, Centre Hospitalier Universitaire, 80 Avenue Augustin Fliche, 34295 Montpellier Cedex 05, France
Manuscript submitted June 17, 2019, accepted June 25, 2019
Short title: CRP and Cachexia in Hematological Malignancies
doi: https://doi.org/10.14740/jh536
| Abstract | ▴Top |
Background: Cachexia is defined as an involuntary loss of weight, characterized by a loss of skeletal muscle mass with or without fat mass loss. It increases mortality risk and decreases quality of life in patients with lymphoma or myeloma. Early markers of cachexia are not identified. The objective of this work was to identify risk factor of cachexia in a cohort of patients with hematological malignancies to develop strategies to prevent cachexia and its consequences.
Methods: Clinical and biological parameters were collected before and at the end of the treatment. Quantification of weight loss during cachexia was performed by the method of Martin. Clinical responses to treatment of patients with lymphoma or myeloma were monitored.
Results: Thirty-eight percent of the 145 patients enrolled were cachectic at the end of treatment. Classical prognostic disease scores at the time of diagnosis seemed to be not associated with cachexia observed at the end of treatment. Only C-reactive protein (CRP) > 54 mg/L seemed to be a risk factor of cachexia (P = 0.023, odds ratio (OR): 5.94 (1.55 - 39.14), confidence interval (CI): 1.55 - 39.14). Those results were confirmed by bootstrap analysis.
Conclusion: This study highlights that high CRP level at diagnosis seems to be a risk factor for cachexia during treatment, permitting to identify patients at risk and in future to implement preventive strategies.
Keywords: Cachexia; Lymphoma; Myeloma; CRP; Inflammation
| Introduction | ▴Top |
Cachexia is defined by an involuntary weight loss that cannot be fully reversed by conventional nutritional support and leads to progressive functional impairment [1]. Weight loss in cancer cachexia can be classified according to Martin et al score [2]. Cachexia is characterized by muscle mass loss with or without fat loss [1] and can be explained by complex phenomena like a decrease in protein synthesis promoting depletion of muscle tissue [1, 3] and an increase in inflammation level [3]. This inflammation is a key marker of cachexia and is characterized by an increase in biochemical markers such as C-reactive protein (CRP), inflammation marker secreted by the liver in response to increase in interleukine-6 (IL-6) level [1, 4, 5]. During hematological malignancies, cachexia concerns more than 30% of patients, with an increase of mortality risk and a decrease of quality of life [6]. The role of chemotherapy in this cachexia either by improving cancer-related cachexia or by inducing cachexia itself is well recognized [1]. Despite identification of mechanisms leading to a loss of muscle mass, the precise identification of cachexia risk factors before cancer treatment remains insufficient and their influence on patient outcome is not defined. Thus, the objective of this work was to identify risk factors of cachexia in myeloma and lymphoma patients, from the outset of cancer diagnosis, to develop strategies to prevent cachexia and its consequences.
| Materials and Methods | ▴Top |
Patients
This study was based on a prospective and observational study (NCT02134574). One hundred forty-five patients diagnosed with lymphoma or myeloma (aged > 18 years) between 2014 and 2017 were enrolled and completed their treatment. This cohort consisted of a prospective collection of clinical and biological data, from patients consulting for a diagnosis of hematological malignancies within the Department of Clinical Hematology of the Montpellier University Hospital. Clinical responses to treatment of patients were monitored according to international recommendations using prognostic indicators [7, 8] and the disease relapse date was identified to determine progression-free survival (PFS). This study was approved by the Institutional Ethics Committee in accordance with the principles of the Helsinki Declaration (National Agency for the Safety of Medicines and Health Products (ANSM), reference: ANSM 13029B-11 of 21/03/2013, Committee for the Protection of Persons (CPP) Sud mediterranee I, reference: 13 24 of 02/04/2013).
Cachexia diagnosis
Each patient losing weight during treatment was considered cachectic, including cachexia induced by treatment. Cachexia was determined at the end of the hematological treatment. For that, a severity stage between 0 and 4 was attributed according to Martin criteria [2] (where stage 0 is the lowest severity stage and stage 4 is the highest severity stage of cachexia).
Statistical analysis
Distributions of data were tested with the Shapiro-Wilk test. Chi-squared or Fisher’s exact tests were used to compare categorical data. For numerical data, medians were compared using Student’s t-test or Mann-Whitney’s test. Spearman’s correlation test was used to assess the association between two numerical variables. The association between covariates and cachexia was assessed using multivariate logistic regression analysis. The receiver operating characteristics (ROC) curve was used to determine the threshold value to predict cachexia associated with the best sensitivity and specificity according to the Youden index [9]. Results from Cox regression was internally validated using bootstrap procedure [10, 11], generating a total of 1,000 replicates. PFS was measured from the date of the initiation of treatment to the date of relapse and/or progression. PFS was estimated using the Kaplan-Meier method and comparisons were made using the log-rank test. Hazard ratios (HRs) and their 95% confidence intervals (CIs) in univariate and multivariate analyses were calculated using Cox regression analyses. All statistical analyses were performed at the conventional two-tailed α level of 0.05 using R software version 3.0.2.10.
| Results | ▴Top |
Patients
Of the 145 patients, 89 were men and 56 were women. Thirty of patients were diagnosed for Hodgkin’s lymphoma, 84 patients for non-Hodgkin’s lymphoma and 31 for myeloma. All clinical and biological data are shown in Table 1.
 Click to view | Table 1. Clinical and Biological Data at Diagnosis |
Cachexia prevalence
The average time interval between the two weight measurements was 8 months (i.e. treatment time). Fifty-five out of 145 patients (38%) present a cachectic state at the end of treatment (Fig. 1): 11 with a weight loss of severity 0 (7.5% of 145 patients), 17 with a severity 1 (12%), 11 with a severity 2 (7.5%), 13 with a severity 3 (9%) and three with a severity 4 (2%).
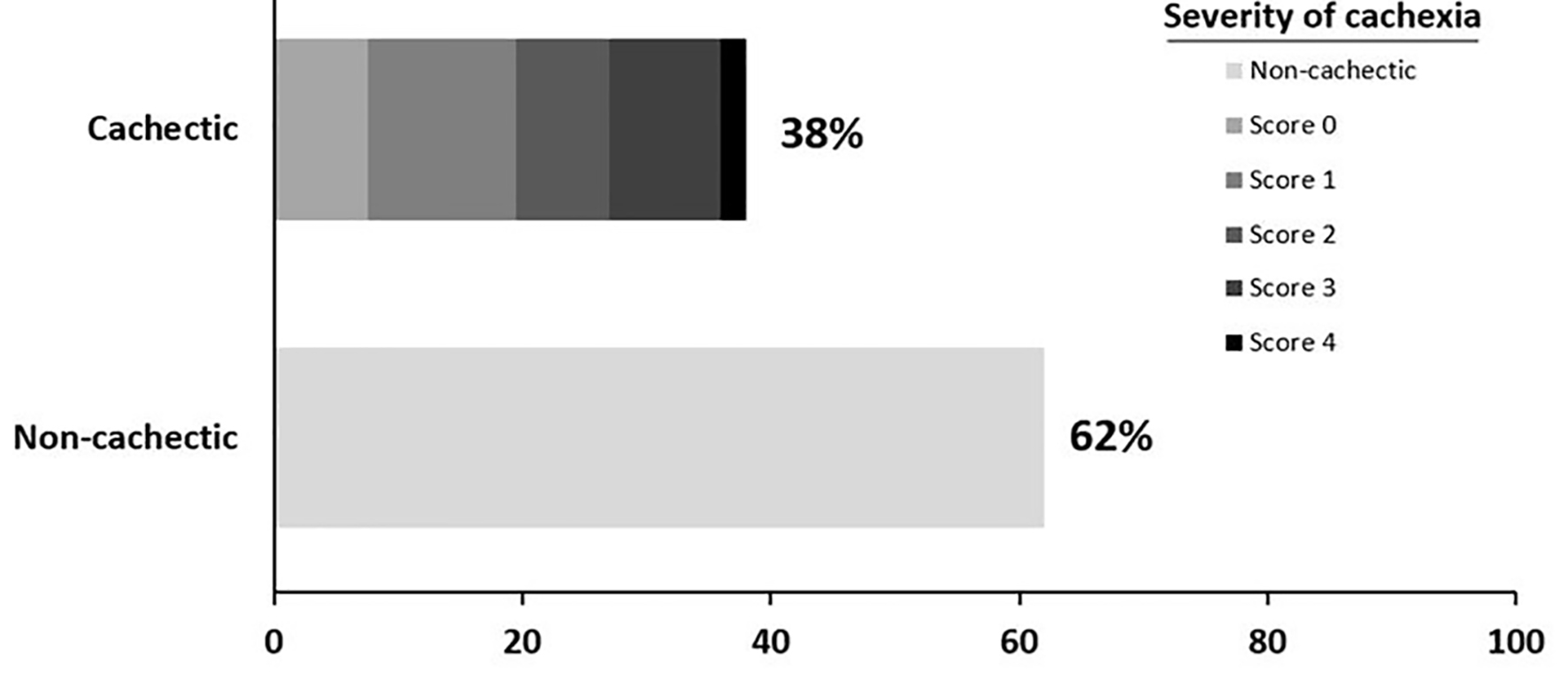 Click for large image | Figure 1. Proportion (%) of the cachectic (n = 55) and the non-cachectic (n = 90) patients. Cachexia prevalence is represented by the score of weight loss severity (score of Martin): weight loss of severity 0 (n = 11), severity 1 (n = 17), severity 2 (n = 11), severity 3 (n = 13) and severity 4 (n = 3). |
Risk factors for cachexia and patients’ outcome
Classic disease prognostic scores were not significantly associated with cachexia (Table 2). Among the biological and clinical data, only CRP seems to be associated with cachexia. The ROC curves were used to determine a threshold value of 54.0 mg/L for CRP level at diagnosis that discriminated between patients who were cachectic or not cachectic during treatment. A CRP level greater than 54.0 mg/L at diagnosis appears to be a risk factor for cachexia during treatment (P = 0.023, odds ratio (OR): 5.94, CI: 1.55 - 39.14). These results were confirmed by bootstrap analyse, and a CRP > 54 mg/L still appears to be a risk factor for cachexia (OR: 8.17, CI: 3.44 - 19.41) (Table 2). Nine patients died as a result of treatment and 34 relapsed (median: 26.3 months; min.: 7.3; max.: 45.0; interquartile range (IQR): 18.5 - 33.2). At diagnosis, CRP > 54 mg/L appears to be a risk factor for relapse (P = 0.012, HR: 2.96, CI: 1.22 - 7.14), as well as Ann Arbor stage (P = 0.033, HR: 0.32, IQR: 0.11 - 0.96).
Click to view | Table 2. Association Between Parameters Measured at Diagnosis and Cachexia During Treatment |
| Discussion | ▴Top |
CRP level at diagnosis: a risk factor for cachexia at the end of treatment of lymphoma or myeloma
High CRP level at cancer diagnosis appears to be a cachexia risk factor for 38% of patients losing weight during hematological treatment. These results are consistent with our bootstrap analysis, but had never been highlighted in hematology. Indeed, the increase in inflammation level, symbolized by an increase in CRP level, is one of the major mechanisms of cachexia that can lead to loss of muscle mass and increase mortality risk [1, 12].
CRP level at diagnosis: a risk factor for relapse of lymphoma or myeloma
In addition, high CRP level at diagnosis appears to be a risk factor for relapse and therefore a risk factor for early mortality. This relationship could reflect a cachexia not previously diagnosed or sarcopenia (i.e. muscle deconditioning linked to advanced age [13]). Indeed, inflammation could reflect sarcopenia development [14] instead of cancer-related cachexia, seeing that the median age of the patients in the present study is 62 years. Finally, a high level of inflammation could also reflect advanced stages in cancer at diagnosis [15]. These data can enable clinicians to identify patients at risk for cachexia and implement preventive strategies to reduce its prevalence.
Limitations
This study presents different limitations or bias. Cachexia was only assessed at the end of treatment. We have no follow-up of the evolution of patients’ weight loss during treatment. Furthermore, we used only weight loss to diagnose cachexia, which can be insufficient [16]. Computed tomography scan or magnetic resonance imaging could be used due to their higher precision about body composition.
Perspectives
In our study, 38% of patients are cachectic during treatment for a lymphoma or a myeloma. Beyond the probable changes in quality of life, we suggest also that these patients can present an increased risk of mortality [2, 17]. With the identification of high CRP level as a diagnostic cachexia risk factor and a relapse risk factor, the implementation of preventive strategies is possible, favorable and recommended [12]. Indeed, cachexia is a phenomenon that is not completely reversible, whose main mechanisms are an increase in the level of inflammation and a negative imbalance in protein synthesis [1]. The practice of physical activity, and particularly adapted physical activity, would be one of the ways to prevent its appearance and is part of the management recommendations [12, 18, 19].
Conclusion
This study has highlighted that high CRP level at diagnosis seems to be a risk factor for cachexia during treatment and a risk factor for relapse.
Acknowledgments
None.
Financial Disclosure
This work is supported by a public grant overseen by the European funds of regional development (reference no.:2015 009260/LR 0001082).
Conflict of Interest
All authors declare that they have no conflict of interest.
Informed Consent
Each patient provided a written informed consent.
Author Contributions
Joris Mallard, Anne Laure Gagez and Guillaume Cartron have written the article. Guillaume Cartron worked on the study design and Pierre Louis Bernard, Aline Herbinet, Jonathan Maury and Cedric Baudinet read and approuve the final manuscript, and help for the results analysis. All authors accepted the final version of the manuscript.
| References | ▴Top |
- Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, Jatoi A, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011;12(5):489-495.
doi - Martin L, Senesse P, Gioulbasanis I, Antoun S, Bozzetti F, Deans C, Strasser F, et al. Diagnostic criteria for the classification of cancer-associated weight loss. J Clin Oncol. 2015;33(1):90-99.
doi pubmed - Aoyagi T, Terracina KP, Raza A, Matsubara H, Takabe K. Cancer cachexia, mechanism and treatment. World J Gastrointest Oncol. 2015;7(4):17-29.
doi pubmed - Evans WJ, Morley JE, Argiles J, Bales C, Baracos V, Guttridge D, Jatoi A, et al. Cachexia: a new definition. Clin Nutr. 2008;27(6):793-799.
doi pubmed - Morley JE, Thomas DR, Wilson MM. Cachexia: pathophysiology and clinical relevance. Am J Clin Nutr. 2006;83(4):735-743.
doi pubmed - Pressoir M, Desne S, Berchery D, Rossignol G, Poiree B, Meslier M, Traversier S, et al. Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br J Cancer. 2010;102(6):966-971.
doi pubmed - Durie BG, Harousseau JL, Miguel JS, Blade J, Barlogie B, Anderson K, Gertz M, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20(9):1467-1473.
doi pubmed - Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, Lister TA, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-3068.
doi pubmed - Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3(1):32-35.
doi - Efron B. Bootstrap methods: another look at the jackknife. Ann Stat. 1979;7:1-26.
doi - Efron B, Tibshirani R. Bootstrap methods for standard errors, confidence intervals, and other measures of statistical accuracy. Stat Sci. 1986;1:54-75.
doi - Gould DW, Lahart I, Carmichael AR, Koutedakis Y, Metsios GS. Cancer cachexia prevention via physical exercise: molecular mechanisms. J Cachexia Sarcopenia Muscle. 2013;4(2):111-124.
doi pubmed - Muscaritoli M, Anker SD, Argiles J, Aversa Z, Bauer JM, Biolo G, Boirie Y, et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: joint document elaborated by Special Interest Groups (SIG) "cachexia-anorexia in chronic wasting diseases" and "nutrition in geriatrics". Clin Nutr. 2010;29(2):154-159.
doi pubmed - Bowen TS, Schuler G, Adams V. Skeletal muscle wasting in cachexia and sarcopenia: molecular pathophysiology and impact of exercise training. J Cachexia Sarcopenia Muscle. 2015;6(3):197-207.
doi pubmed - Marelli G, Sica A, Vannucci L, Allavena P. Inflammation as target in cancer therapy. Curr Opin Pharmacol. 2017;35:57-65.
doi pubmed - Roeland EJ, Ma JD, Nelson SH, Seibert T, Heavey S, Revta C, Gallivan A, et al. Weight loss versus muscle loss: re-evaluating inclusion criteria for future cancer cachexia interventional trials. Support Care Cancer. 2017;25(2):365-369.
doi pubmed - Farkas J, von Haehling S, Kalantar-Zadeh K, Morley JE, Anker SD, Lainscak M. Cachexia as a major public health problem: frequent, costly, and deadly. J Cachexia Sarcopenia Muscle. 2013;4(3):173-178.
doi pubmed - Antoun S, Raynard B. Muscle protein anabolism in advanced cancer patients: response to protein and amino acids support, and to physical activity. Ann Oncol. 2018;29(suppl_2):ii10-ii17.
doi pubmed - Radbruch L, Elsner F, Trottenberg P, Strasser F, Fearon K. Clinical practice guidelines on Cancer Cachexia in advanced cancer patients. Eur Palliat Care Resarch Collab. 2010.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.